Sacroiliac Tumor Resection: A Case Study in Patient-Specific Cutting Guide Design
- Isabelle Têcheur
- May 12
- 2 min read







Sacroiliac tumor resection is one of the most demanding procedures in orthopedic oncology. At the junction between the ilium and the sacrum, the surgical field is dense with vascular and neural structures. Combining preoperative 3D planning with a patient-specific cutting guide gives the surgical team a way to define every cutting plane, every trajectory and every safety margin before the procedure.
This article reviews a recent sacroiliac tumor resection performed by Dr Valérie Dumaine at APHP Cochin (Paris).
Preoperative Planning
The resection plan was built on a 3D reconstruction of the patient’s pelvis, generated from preoperative CT and MRI scans. The plan included:
• Six cutting planes opening surgical access to the tumor
• A 10 mm safe margin on the ilium
• A 7 mm safe margin on the sacrum
• A posterolateral approach
• A deliberately oblique sacral cutting plane, chosen to pass between the tumor volume and the nearby sacral nerve roots
Each parameter was discussed and validated with the surgeon before any instrument was manufactured. The oblique sacral plane was the geometry that respected the tumor margin while keeping the sacral nerve roots outside the resection volume.
The Patient-Specific Cutting Guide
Dr Dumaine then applies this plan in the operating room with the help of the patient-specific guide. Designed from the patient’s own anatomy, the guide fits the bone in a single supporting position. From this reference, the surgeon directs the Kirschner wires and the saw blade along the validated cutting paths.
For this case, two guides were produced: one for the iliac side, and one positioned on the posterior sacrum.
The sacral guide integrates two parallel Kirschner wires from the planning stage. These pins serve two purposes:
• They anchor the guide in its planned position on the bone.
• They act as a stable reference if an intraoperative laminectomy is required.
If, during the procedure, the surgeon needs to open the sacral canal to access the nerve roots, she can slide the guide off, perform the laminectomy, and slide the guide back over the same parallel pins. The guide returns to its preoperative position without any new alignment step, preserving the precision of the original plan and leaving the surgeon full intraoperative flexibility.
Outcome
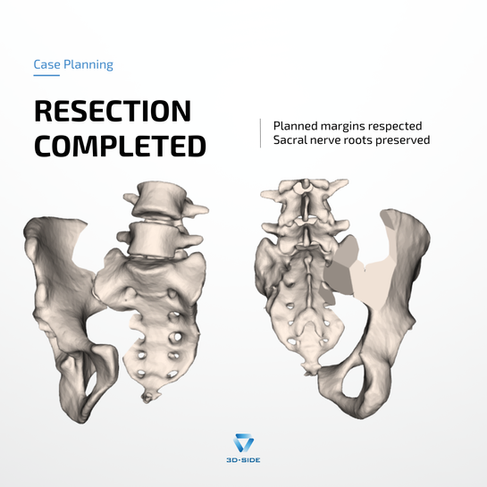
The sacroiliac tumor resection was performed according to the validated plan. Planned margins were respected. Sacral nerve roots were preserved.
The case illustrates the value of patient-specific instrumentation in anatomically constrained configurations: a clear plan defined in advance, with the geometry and the safety features already built into the instrument before it reaches the operating room.
3D-Side designs and manufactures patient-specific cutting guides for orthopedic oncology, in close collaboration with surgical teams worldwide. Contact us to discuss your case.