Bone tumor resection guides: solving a dual-approach iliac chondrosarcoma
- Isabelle Têcheur
- Apr 29
- 2 min read








Preserving the tensor fasciae latae while respecting resection margins — how patient-specific 3D planning made possible what a single guide could not achieve.
Dr. David Blau
Surgeon · Paris, France The surgical challenge: when standard planning falls short
When a chondrosarcoma affects the ilium, the surgical question goes beyond resecting the tumor with sufficient margins. It also includes what the surgeon chooses not to sacrifice and that decision shapes every aspect of the bone tumor resection guide to be designed.
For Dr. Blau, this constraint was set from the planning phase: preserve as much as possible the insertion of the tensor fasciae latae, a key muscle for lower limb stability and function. A decision that in practice entirely reconfigured the instrument architecture.
7mm Planned margin on the acetabular plane
10mm Margin on all other cutting planes
4 Cutting planes · Dual approach · 6 K-wires
Why a single bone tumor resection guide was not enough
The anatomical constraint was clear: the superior cut could not be performed through the lateral approach without compromising the tensor fasciae latae insertion. It had to be approached from the endopelvic side, from inside the pelvis.
This configuration made a single guide structurally impossible — both access routes were incompatible within one instrument. A patient-specific dual-guide system was the only viable solution.
Patient-specific dual-guide design: how it works
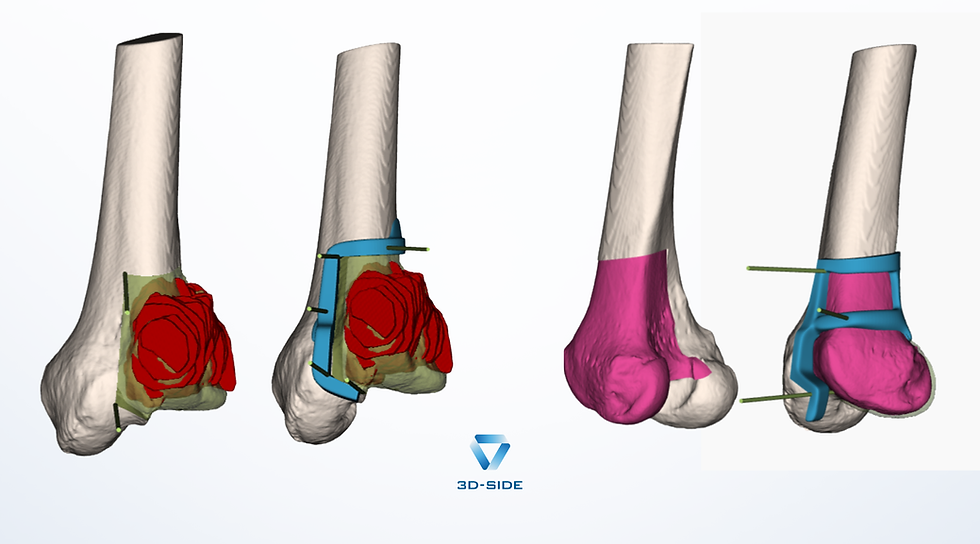
The solution was to design two distinct but interdependent guides whose sequential placement guarantees the precision of each cut.
The lateral guide is positioned first, fixed to the bone with K-wires that pass through the cortex and exit on the endopelvic side. One single fitting position on the bone ensures optimal reproducibility.
The endopelvic guide slides over the same K-wires exiting through the lateral guide, finding its own single fitting position. Both instruments are connected and all cutting planes are set.
Guide stability was refined iteratively with the surgeon: the anterior and inferior wings were enlarged to ensure more reliable contact with the pelvic anatomy. The final version was validated before the procedure.
Outcome: margins respected, function preserved
The resection was completed according to the preoperative plan, four cutting planes, dual approach, six K-wires. Resection margins were respected and the tensor fasciae latae was preserved.
This case demonstrates how patient-specific bone tumor resection guides can go beyond adapting a standard instrument: they can require rethinking the entire guide architecture to meet anatomical and functional constraints that initially seemed irreconcilable.
Key takeaway for surgical planning
Functional preservation can be built into the instrument design from the start not treated as a secondary constraint. When anatomy demands it, two interdependent patient-specific guides can accomplish what a single bone tumor resection guide cannot, provided planning is rigorous enough to anticipate every operative step.

Comments