Grade 2 Iliac Chondrosarcoma: Extra-Articular Resection and Reconstruction with Patient-Specific Instrumentation
- Isabelle Têcheur
- May 27
- 2 min read
Updated: May 28

Extra-articular resection of a grade 2 iliac chondrosarcoma via ilioinguinal approach, with patient-specific cutting and reconstruction guides from a single 3D planning session. When a chondrosarcoma extends deep into the ilium and reaches the acetabulum, the surgical question goes beyond resection margins. The location itself dictates hip reconstruction, and that decision needs to be built into the planning from the start, not treated as a secondary step.
Preoperative Planning
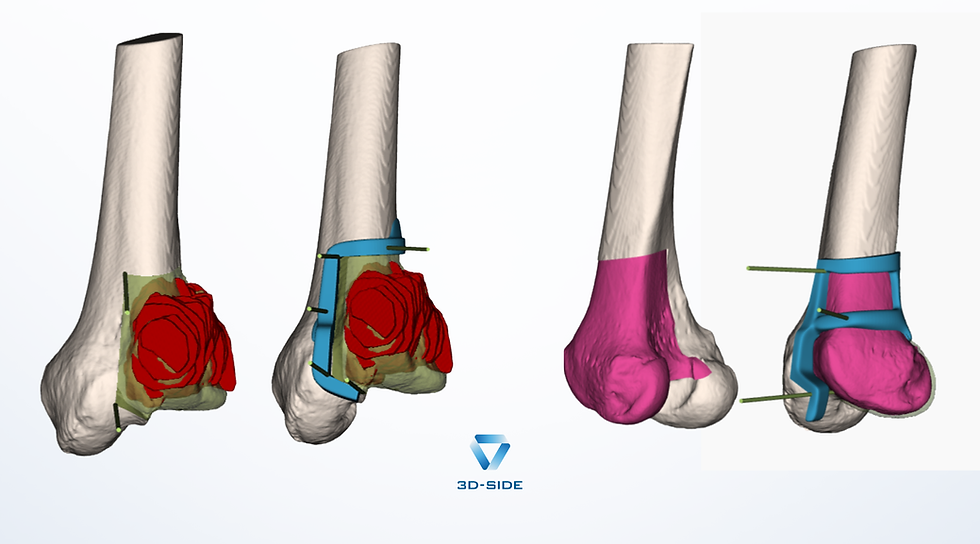
The plan is built on a 3D reconstruction of the pelvis (CT and MRI). Three cutting planes are defined: a 10 mm margin on the main planes, and a 7 mm margin on the posterior column, deliberately chosen to preserve more bone and maintain a stronger pelvis after the procedure. The ilioinguinal approach is selected for optimal exposure of the tumor volume.
The resection is extra-articular, and the hip joint is replaced by the Ice-cream cone implant.
The patient-specific cutting guide is designed for the lateral approach and fixed with three 2.0 mm Kirschner wires. Its wings guarantee a single fitting position on the bone and ensure stability throughout the osteotomy.
It is the guide geometry that translates the plan into a surgical gesture: every parameter is already resolved before the patient enters the operating room.
10 mm · Primary margin 7 mm · Posterior column 3 · Cutting planes
Ice-Cream Cone Reconstruction Guide
A second patient-specific guide is designed to direct the stem of the Ice-cream cone implant. It rests on the iliac wing surface and on the cutting surfaces from the resection, the same geometric references as the first guide.
This continuity between the two instruments is what ensures consistency across the entire procedure, from the first cutting plane to the final implant positioning.
Outcome
The extra-articular resection was performed according to the validated plan, with oncological margins respected across all cutting planes. The reconstruction guide enabled precise positioning of the implant stem in line with the planned parameters.
Key takeaway
In complex pelvic cases, anticipating reconstruction from the resection planning phase is not optional: it is what allows both operative stages to share the same geometric consistency.

Comments