When proximal femoral correction must align with intramedullary fixation
- Isabelle Têcheur
- Feb 25
- 2 min read









A staged, patient-specific strategy
This case represents the second surgical stage of a bilateral femoral correction performed in close collaboration with Drs. Gabriel T. Mindler, Catharina Chiari, and Benjamin Kraler at the Orthopedic Hospital Speising in Vienna, as part of the Vienna Bone and Growth Center, a specialized center for rare bone diseases.
The patient presented with fibrous dysplasia, characterized by complex femoral deformities, requiring a staged and patient-specific treatment strategy. In this context, 3D planning was preferred over a freehand approach to enable precise bone resection with optimal contact of the resection surfaces, aiming to promote the best possible bone healing in this rare bone disease.
After correction of the right femur, the left side required a dedicated approach while maintaining the same objectives of accuracy and reproducibility.
The surgical focus was limited to the proximal femur. The deformity was multiplanar, combining angular and rotational components, with the additional challenge of ensuring full compatibility between deformity correction and intramedullary nail insertion.
Integrating correction and fixation
Based on predefined clinical and biomechanical considerations, a partial correction of the neck–shaft angle and femoral rotation was intentionally targeted, with the correction precisely defined preoperatively.
In parallel, achieving a reliable and reproducible intramedullary nail trajectory was a central objective. Proximal correction alone was not sufficient to achieve this.
The planning strategy was therefore extended to actively guide both the entry point and axis of a custom-made intramedullary nail.
A detailed 3D planning process enabled the design of a patient-specific corrective osteotomy combined with dedicated instrumentation.
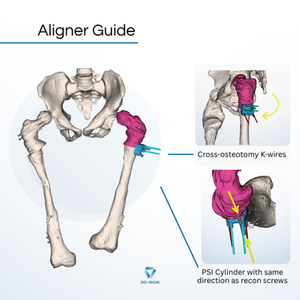
A cutting guide ensured accurate reproduction of the planned osteotomy planes, while alignment K-wires, maintained the correction during nail insertion in combination with an aligner guide.
The same guide allowed placement of two cross-osteotomy K-wires, further stabilizing the correction throughout fixation.
To facilitate controlled insertion and accurate alignment of the custom-made nail through the distal femoral fragment, a dedicated entry-point guide was designed to guide a drill that pre-drills the nail entry point in the distal femoral fragment, thereby easing nail insertion and ensuring that the nail axis corresponds to the preoperative plan.
As with the contralateral side, this case highlights the importance of aligning correction geometry, fixation strategy, and implant insertion through close collaboration between planning and surgical execution.
We sincerely thank Dr. Gabriel T. Mindler and the entire surgical team for their trust, continuous input during planning, and precise execution of this demanding bilateral correction


Comments