Bone Tumor Resection Planning: A Case of Maximum Bone Preservation
- Isabelle Têcheur
- Mar 26
- 2 min read


"Low grade lesion, we need to keep the maximum of bone."
These were the words Dr. Ropars used to validate the resection plan for this case of scapular spine bone tumor.
A short sentence. A decision that captures the full complexity of orthopedic oncology surgery.
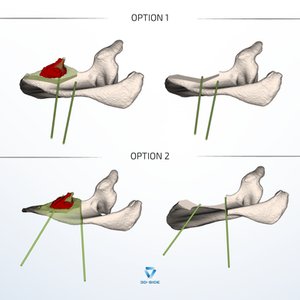
Faced with this case, our team proposed two resection options to the surgeon:
Option 1: superoposterior approach, 5 mm margin, guide positioned on the superior border of the spine, floating medially above the supraspinous fossa. More complex to design. But with the tumor located anteriorly, this approach allows access without sacrificing healthy bone tissue.
Option 2: conventional posterior approach, 10 mm margin, guide placed directly on the scapular blade. Safe. Standard.
Dr. Ropars chose Option 1. Because with a low-grade lesion, the goal is not only to achieve clean margins, it is also to preserve bone, function, and the patient's long-term quality of life.
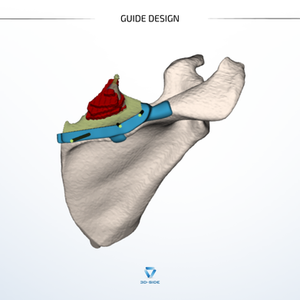
Once the planning is validated, the real design work begins.
And that is where constraints become tangible.
Example: the lateral vertical resection plane initially had a 5 mm margin. Oncologically sound on paper. But when integrating the geometry of all three planes, our engineer identified that this reduced the effective width of the intermediate oblique cutting plane, making it too narrow for a saw blade to work reliably.
The solution proposed to Dr. Ropars:
— Increase the lateral margin to 10 mm to allow all three cuts to be made with the guide in place
— Or keep 5 mm, remove the guide after the first two planes, and complete the third freehand
His choice: keep the guide for all three cuts, with the adapted margin. The safety of a guided gesture took precedence over the additional millimeter of bone preservation.
The same logic applied to guide fixation: two possible support zones were proposed, one optimized for stability, the other minimizing interference with the exposed soft tissues. A choice that does not exist with a standard guide, because a standard guide does not know this patient's anatomy.
This continuous dialogue between clinical judgment and engineering is what defines our approach at 3D-Side. Every technical decision is submitted to the surgeon. Every intraoperative constraint is anticipated before the OR.
Thank you to Dr. Mickaël Ropars and the team at CHU Rennes - Pontchaillou for their trust and collaboration.


Comments